
Beyond Cholesterol Reduction: Understanding What Really Drives Heart Disease
Beyond Cholesterol Reduction: Understanding What Really Drives Heart Disease
Cholesterol Matters, But It’s Not the Whole Story
Dr John Sciales
Director: CardioCore Metabolic Wellness Center
Summary
For decades, heart disease prevention focused mainly on lowering cholesterol, especially LDL cholesterol. While cholesterol remains important and statins have helped save many lives, modern research now suggests that heart disease is far more complex than cholesterol alone. Increasingly, cardiovascular disease is being understood as a chronic inflammatory and metabolic disease involving the artery wall itself.
This article explores how inflammation, insulin resistance, oxidative stress, metabolic dysfunction, plaque biology, and lifestyle factors such as sleep, stress, nutrition, and exercise may all influence the development and progression of heart disease. It also explains why many heart attacks occur despite “normal” cholesterol levels and how modern imaging techniques can help identify disease more directly inside the arteries.
Most importantly, this article introduces a more proactive and personalized approach to prevention, one that focuses not only on cholesterol reduction, but also on understanding and addressing the underlying biologic drivers of vascular injury and chronic disease.
The purpose of this article is to shift the conversation away from simply asking, “What is my cholesterol?” and toward asking more important questions:
“Do I actually have heart disease?”
“What is driving my plaque biology?”
“What is happening metabolically beneath the surface?”
Because cholesterol may suggest risk, but understanding the biology inside the artery may help define the disease itself.
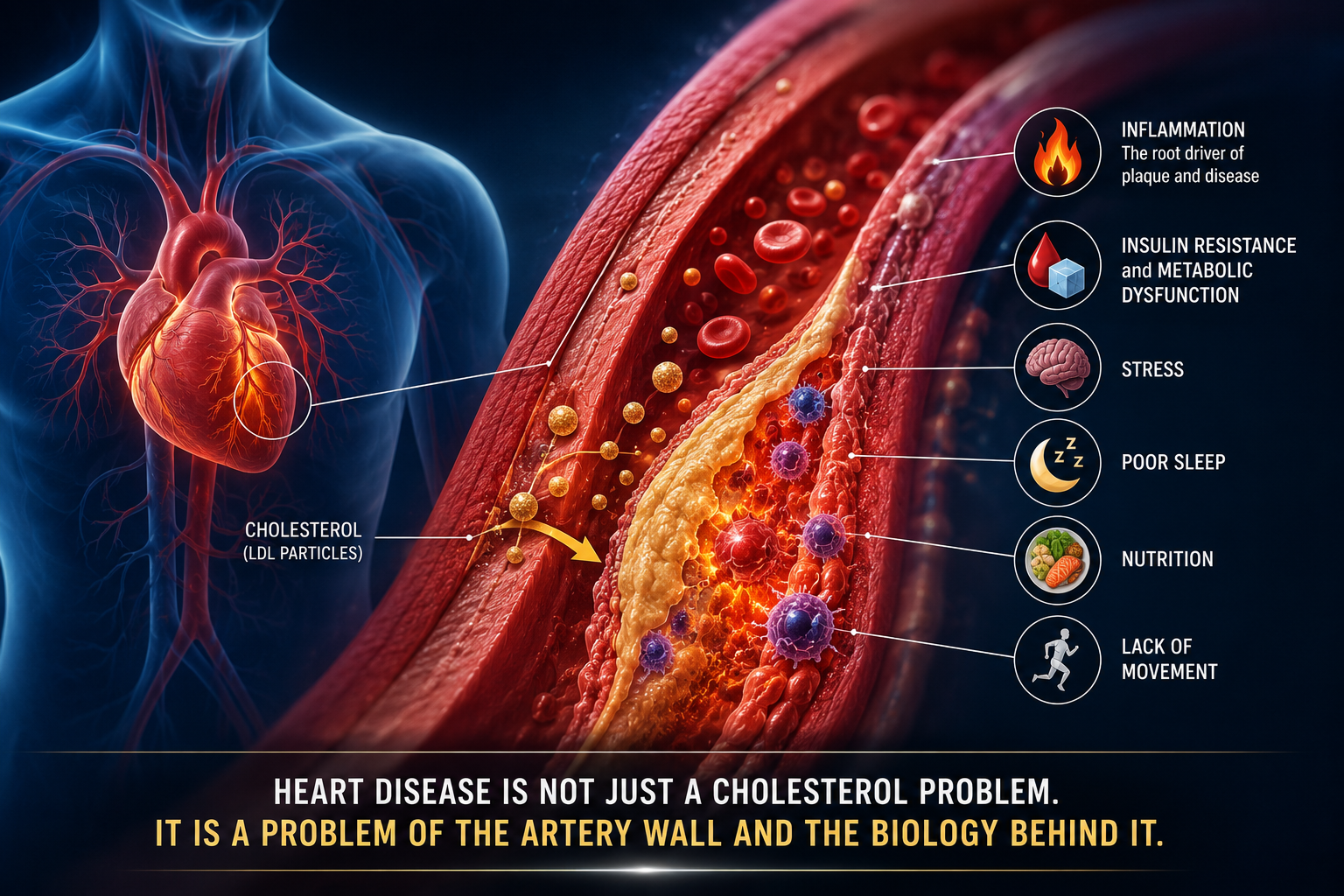
Figure 1. Modern cardiovascular disease is increasingly understood as a chronic inflammatory and metabolic disease of the artery wall rather than simply a disorder of elevated cholesterol alone. Plaque behavior is influenced by inflammation, insulin resistance, oxidative stress, stress physiology, sleep, nutrition, and overall metabolic health.
Why Cholesterol Alone Doesn’t Explain Heart Disease
For many years, heart disease was viewed mainly as a cholesterol problem. Doctors focused heavily on lowering LDL cholesterol, often called “bad cholesterol,” because research clearly showed that people with higher LDL levels had greater risk for heart attacks and strokes. Medications called statins became a major breakthrough in cardiovascular medicine and have helped save many lives, especially in people who already have known heart disease.(1–4)
During the 1990s and early 2000s, major direct-to-consumer pharmaceutical advertising further reinforced the idea that cholesterol was the central focus of heart disease prevention. Millions of people became familiar with their cholesterol numbers and were encouraged to ask their doctors, “What’s my cholesterol?” In many ways, cholesterol became one of the most recognized laboratory values in medicine.
However, LDL is not actually “cholesterol” itself. LDL stands for low-density lipoprotein, which is a carrier particle that transports cholesterol, triglycerides, and other lipids through the bloodstream. Cholesterol is only one component of the LDL particle. Over time, however, the terms “LDL” and “cholesterol” became almost interchangeable in everyday conversation, even though LDL is technically a lipoprotein rather than cholesterol itself.
In large population-based studies, higher LDL levels were associated with greater cardiovascular risk across groups of people. However, over time this population-level association sometimes became oversimplified into the idea that cholesterol alone completely explained heart disease in every individual patient. Yet real-world clinical experience increasingly showed that cardiovascular disease behaved far more differently and far more complexly than cholesterol numbers alone would predict.
Doctors and researchers began noticing something important: many people who suffered heart attacks did not have extremely high cholesterol levels. Some patients even had “normal” cholesterol numbers. At the same time, others with elevated cholesterol sometimes showed very little plaque inside their arteries.
This raised an important question: if cholesterol were the entire story, why would heart disease behave so differently from one person to another?
Modern research now suggests that heart disease is much more complex than simply having “high cholesterol.” Increasingly, cardiovascular disease is being understood as a chronic inflammatory and metabolic disease involving the artery wall itself.(5–8)
In other words, cholesterol matters, but the environment surrounding the cholesterol may matter just as much.
The Artery Is Alive
Arteries are not simple plumbing pipes. They are living tissues that constantly respond to stress, inflammation, blood sugar changes, blood pressure, toxins, smoking, processed foods, poor sleep, chronic stress, and metabolic health.
Over many years, these factors can injure the inner lining of the artery, called the endothelium. Once the artery becomes irritated and inflamed, cholesterol particles are more likely to enter the vessel wall and become trapped there.
This changes the way we think about plaque.
Plaque may not simply be “cholesterol buildup.” Instead, plaque may represent the body’s response to years of injury, inflammation, oxidative stress, blood sugar problems, insulin resistance, and abnormal metabolic signaling.(8,10,11)
In many ways, cholesterol may act more like fuel being added to an already inflamed artery rather than the only cause of disease itself.
Why Inflammation Matters
Inflammation has become one of the biggest new discoveries in heart disease.
Scientists now understand that inflammation plays a major role in plaque formation, plaque growth, plaque instability, and heart attacks themselves.(5–8)
Some plaques become “vulnerable plaques,” meaning they are more likely to rupture or erode and suddenly form blood clots that block blood flow to the heart.
Importantly, many heart attacks occur in plaques that were not severely blocked beforehand. In fact, many dangerous plaques may appear only “mild” on testing before they suddenly rupture.(9) More heart attacks occur from plaque rupture and plaque erosion than from the slow gradual closure of an artery itself. In many cases, a sudden plaque rupture followed by rapid clot formation can produce a major heart attack with far more serious consequences than slowly progressive narrowing alone.
This was a major shift in cardiovascular medicine because it showed that the most dangerous plaque is not always the plaque causing the biggest blockage. Sometimes the most dangerous plaque is the most inflamed and biologically unstable plaque.
That is why inflammation, oxidative stress, insulin resistance, and metabolic health are now receiving far more attention in preventive cardiology.
Heart Disease and Metabolic Health Are Deeply Connected
Today, doctors are seeing enormous increases in obesity, insulin resistance, type 2 diabetes, fatty liver disease, high triglycerides, poor sleep, chronic stress, and The Metabolic Syndrome.(10,11)
Many patients with heart disease also have elevated triglycerides, low HDL cholesterol, belly fat, abnormal blood sugar, elevated insulin levels, high blood pressure, or chronic fatigue. Often, these problems exist for years before diabetes is officially diagnosed.
In fact, insulin resistance may quietly damage blood vessels long before blood sugar becomes even mildly abnormal.(10,16) Increasing evidence suggests that metabolic dysfunction and insulin resistance are often present years before patients are formally diagnosed with diabetes mellitus. Elevated blood sugar is often a relatively late manifestation of insulin resistance, whereas coronary artery disease may represent one of its earlier and more dangerous consequences. Importantly, this process often develops silently below the radar and may remain completely undetected unless specifically evaluated through more advanced metabolic assessment and cardiovascular testing.
Studies evaluating patients with cardiovascular disease have shown that many individuals without known diabetes already demonstrate abnormal glucose metabolism or insulin resistance when more advanced metabolic testing is performed. In many respects, elevated blood sugar itself may represent a relatively late manifestation of a much longer underlying process involving insulin resistance, metabolic dysfunction, inflammatory activation, and vascular injury.
This is one reason why many experts now believe that heart disease cannot be fully understood by cholesterol numbers alone. The body’s overall metabolic health strongly influences how arteries behave.
Looking Beyond the Cholesterol Number
One of the biggest changes in modern heart care is the growing use of imaging tests that actually look at the arteries themselves.
A CT Coronary Calcium Scan, often called a CAC score uses low dose CT scanning to identify calcium buildup inside the coronary arteries long before symptoms appear. More advanced imaging, such as coronary CT Angiography (CCTA), can evaluate further including plaque characteristics and plaque “behavior.”(12)
This represents an important shift in medicine. For many years, LDL cholesterol levels and cardiac stress testing were among the primary tools available to evaluate cardiovascular risk before symptoms developed. However, LDL cholesterol alone is a relatively poor predictor of which individual patients actually have plaque inside their arteries, while stress tests generally do not detect early heart disease itself. Instead, stress testing primarily detects later-stage disease in which plaque has already progressed enough to significantly reduce blood flow to the heart.
In other words, many people may have substantial plaque buildup despite a “normal” stress test because the artery may not yet be severely blocked enough to reduce blood flow during exercise.
One of the most well-known examples often discussed in cardiology was Tim Russert, longtime host of Meet the Press, who reportedly had a normal stress test and LDL cholesterol below 70 mg/dL before suddenly dying from a heart attack at age 58. His case became widely discussed because it highlighted an important reality of cardiovascular disease: severe events may still occur despite “acceptable” cholesterol numbers and previously normal stress testing when biologically vulnerable plaque is already present within the arteries.
Cholesterol may suggest risk.
But imaging can show actual disease.
Two people with the exact same cholesterol level may have completely different amounts of plaque inside their arteries.
That is why many doctors now believe that understanding the artery itself is often more important than relying on cholesterol numbers alone.
Why Some People Still Have Heart Attacks Despite “Good” Cholesterol
One of the biggest surprises in modern cardiology is that many people who suffer heart attacks already have LDL cholesterol levels considered “controlled” or “normal.” Some patients are even taking cholesterol medications when cardiovascular events still occur.
This does not mean cholesterol is unimportant. Cholesterol still matters, especially LDL and ApoB-containing particles. However, it does suggest that cholesterol alone does not fully explain why plaque becomes dangerous.
Researchers now believe that inflammation, insulin resistance, oxidative stress, blood sugar abnormalities, high blood pressure, smoking, poor sleep, chronic stress, and metabolic dysfunction may all influence how plaque behaves inside the artery wall.(5–8,10,16)
In other words, cholesterol may help form plaque, but inflammation and metabolic dysfunction may help determine whether plaque remains stable or becomes dangerous.
Importantly, cholesterol itself is not inherently “bad.” Cholesterol is a critically important molecule used throughout the body. It helps form cell membranes, supports hormone production, contributes to brain and nerve function, participates in bile acid formation for digestion, and plays an important role in cellular energy pathways and overall biologic function. In healthy metabolic environments, cholesterol performs many essential physiologic roles.
However, within an unhealthy inflammatory and metabolic terrain characterized by oxidative stress, insulin resistance, chronic inflammation, smoking, poor nutrition, and endothelial injury, lipoproteins may become oxidized and biologically dysfunctional, contributing more directly to plaque instability and vascular injury.
This may help explain why some individuals with elevated cholesterol develop significant cardiovascular disease, while others with relatively similar cholesterol levels develop little plaque and sometimes even demonstrate exceptional longevity. Increasingly, many experts believe that the metabolic and inflammatory environment surrounding cholesterol may substantially influence whether lipoproteins remain relatively stable and physiologic or become biologically harmful within the artery wall.
This is sometimes called “residual risk,” meaning that even after cholesterol improves, other biologic problems may continue damaging the arteries.(5–8)
Plaque Is About More Than Blockage
For many years, cardiology focused heavily on how blocked an artery became. Severe blockages often led to procedures such as stents or bypass surgery.
But modern imaging has changed this understanding.
Doctors now know that many heart attacks occur in plaques that are not severely narrowed before they rupture.(9) Some plaques may only appear “mild” or “moderate” on testing, yet still carry significant danger because of inflammation and instability inside the plaque itself.
This changed the entire way many specialists think about heart disease.
The most dangerous plaque is not always the biggest plaque. Sometimes the most dangerous plaque is the most inflamed plaque.
Traditional stress testing primarily evaluates whether plaque has narrowed the artery enough to reduce blood flow to the heart. In many ways, stress testing mainly identifies later-stage “flow-limiting” disease. However, newer imaging techniques such as coronary CT angiography (CCTA) can evaluate plaque biology itself, including plaque composition, plaque behavior, fibrofatty plaque burden, and biologically high-risk features such as low-attenuation plaque.(9,15)
Advanced imaging studies have shown that some plaques contain large fatty cores, inflammation, immune-cell activity, and unstable tissue that make them more likely to rupture. Other plaques may become more calcified and stable over time.(9,15)
One way to think about this is through the analogy of the Chernobyl disaster nuclear reactor. After the accident, the damaged reactor was covered with massive amounts of concrete to contain the danger beneath it. Similarly, coronary CT imaging can sometimes help doctors understand not only how much “concrete” or calcified plaque is present inside the artery, but also how much biologically active “nuclear material” may still exist underneath the surface in the form of inflamed fibrofatty plaque and unstable low-attenuation plaque. In many respects, the scan is helping physicians evaluate not only how much plaque exists, but how biologically “hot” or unstable that plaque may actually be.
This is why plaque biology matters so much.
Statins Help, But They Are Not the Whole Story
Statins remain one of the most important medications in cardiovascular medicine. They clearly reduce heart attacks, strokes, and cardiovascular death in many patients, especially people who already have established heart disease.(1–4)
But scientists now believe statins may help through more than cholesterol lowering alone.
Research suggests statins may also reduce inflammation, improve endothelial function, stabilize plaque, and lower inflammatory activity inside the artery wall.(13,17)
One important study called the JUPITER trial showed that patients with elevated inflammation markers benefited from statin therapy even when their cholesterol levels were not dramatically elevated.(13)
This helped doctors realize that inflammation itself may be an important treatment target in cardiovascular disease.
Importantly, modern cholesterol guidelines from the American Heart Association and American College of Cardiology shifted significantly in 2013 away from focusing only on achieving a final LDL number.(2) Instead, the guidelines emphasized overall cardiovascular risk, the presence of established atherosclerotic disease, and the use of appropriate moderate- or high-intensity statin therapy according to patient risk category. In many respects, this represented recognition that the cardiovascular benefits of statins may involve more than simply reaching a specific cholesterol target and may also relate to plaque stabilization, inflammatory reduction, endothelial effects, and broader biologic benefits.
However, many patients in real-world practice are still treated using older, pre-2013 “treat-to-number” thinking. Some individuals with known coronary artery disease remain on only low- or moderate-dose statins simply because their LDL cholesterol appears “controlled.” Yet according to established modern guidelines, patients with significant cardiovascular disease often warrant moderate- or high-intensity statin therapy regardless of whether the LDL number already appears relatively low.(2)
At the same time, lowering LDL cholesterol alone does not automatically mean that plaque has disappeared or that the artery has completely healed.
This became particularly important in studies evaluating plaque biology directly with advanced coronary CT imaging. In the EVAPORATE trial, patients receiving statin therapy alone still demonstrated progression of certain high-risk plaque features over time despite relatively well-controlled LDL cholesterol.(15) Over 18 months, fibrofatty plaque volume increased substantially by 32%, while low-attenuation plaque, considered one of the more biologically unstable and higher-risk plaque characteristics,also progressed significantly by 109% in the statin-treated group.
However, in the same patient population, those receiving purified EPA omega-3 therapy called icosapent ethyl demonstrated very different plaque behavior. In these patients, fibrofatty plaque volume decreased by approximately 34%, while low-attenuation plaque decreased by approximately 17%, despite no additional change in LDL cholesterol itself.(15)
These findings were highly important because they suggested that plaque biology may continue evolving even when cholesterol numbers improve and that therapies affecting inflammation, oxidative stress, membrane stability, and plaque behavior may influence cardiovascular risk beyond LDL reduction alone.
Some patients continue developing plaque despite “good” cholesterol numbers because the underlying inflammatory and metabolic environment may still be active. Lowering LDL cholesterol is not necessarily the same as improving the broader inflammatory-metabolic terrain affecting the artery wall itself.
That is why modern cardiovascular prevention increasingly focuses not only on cholesterol reduction, but also on improving inflammation, insulin resistance, oxidative stress, endothelial health, metabolic function, lifestyle factors, and the overall biologic environment within the body.
The Connection Between Insulin Resistance and Heart Disease
One of the most overlooked drivers of cardiovascular disease may be insulin resistance.
Insulin resistance occurs when the body no longer responds properly to insulin, forcing the pancreas to produce higher and higher insulin levels to keep blood sugar under control.
Long before diabetes develops, insulin resistance may contribute to inflammation, high triglycerides, weight gain, fatty liver disease, high blood pressure, oxidative stress, abnormal blood vessel function, and plaque formation.(10,16)
Many people may have insulin resistance for years while their routine blood sugar tests still appear “normal.” In many individuals, insulin resistance represents a chronic low-grade inflammatory state that may silently develop for 10–20 years before blood sugar levels become clearly abnormal. During this time, metabolic dysfunction may gradually damage blood vessels and affect multiple organs throughout the body, including the heart, brain, kidneys, liver, and nervous system.
Importantly, many experts now believe that much of the cardiovascular danger associated with type 2 diabetes may relate less to elevated glucose itself and more to the underlying insulin resistance, inflammatory activation, oxidative stress, endothelial dysfunction, and metabolic injury that often exist long before diabetes is officially diagnosed.
This helped explain why several major diabetes trials, including UKPDS, ACCORD trial, ADVANCE trial, and VADT trial, demonstrated that simply lowering blood sugar alone did not necessarily produce the dramatic cardiovascular risk reduction many expected. Increasingly, these studies suggested that improving the broader metabolic terrain and underlying insulin resistance may be critically important in reducing long-term cardiovascular risk.
This is important because the body may already be experiencing artery damage even before diabetes is officially diagnosed.
In today’s world, many experts now believe that heart disease and metabolic disease are deeply connected.
The artery is not isolated from the rest of the body. The same biologic processes affecting metabolism, body weight, inflammation, stress hormones, sleep quality, and blood sugar also affect the health of the arteries.
Heart Disease Is Often a Whole-Body Problem
Modern medicine is increasingly recognizing that heart disease is not simply a problem of cholesterol floating in the bloodstream. Instead, it may represent the long-term effects of stress, inflammation, poor metabolic health, unhealthy nutrition, sedentary lifestyle, sleep dysfunction, smoking, environmental exposures, and abnormal biologic signaling acting together over many years.(5–11)
In many ways, the artery reflects the overall health of the body.
This helps explain why improving cardiovascular health often requires much more than simply changing one laboratory number.
True prevention may involve improving the entire biologic environment surrounding the artery itself.
In a sense, a CT coronary calcium score not only helps determine whether plaque is present inside the arteries, but may also provide insight into the cumulative inflammatory and metabolic burden the body has experienced over time. The amount of plaque present, particularly when compared with others of similar age and gender, may reflect far more than simply cholesterol exposure alone. In many respects, coronary plaque can be viewed as a visible structural footprint of years of underlying biologic stress and inflammatory response occurring silently beneath the surface.
In this way, the artery becomes a kind of “window” into the body’s deeper inflammatory and metabolic health.
A More Complete Approach to Prevention
This does not mean cholesterol should be ignored. Cholesterol still plays an important role in heart disease, and many patients clearly benefit from statins and other cholesterol-lowering therapies. Patients should never stop medications without speaking with their physician.
But modern cardiovascular medicine is increasingly moving toward a more complete understanding of disease.
The goal is no longer simply lowering a cholesterol number. The goal is understanding whether heart disease is actually present and, if so, why the artery became unhealthy in the first place.
That means looking at the whole picture, including inflammation, blood sugar control, insulin resistance, body composition, sleep quality, stress levels, nutrition, physical activity, blood pressure, smoking history, metabolic health, and even gut health. Many of the same factors that affect energy, weight gain, fatigue, diabetes, and overall wellness also affect plaque formation and artery health.
Importantly, modern guidelines from the American College of Cardiology and American Heart Association increasingly recognize that cholesterol itself is a risk factor rather than the disease itself.(2,12) This is one reason why coronary artery calcium scoring has become increasingly important in patients with elevated cholesterol or intermediate cardiovascular risk but no clearly established heart disease.
For decades, many people with elevated cholesterol were automatically placed on statin therapy without ever determining whether plaque was actually present inside their arteries. Today, advanced imaging is changing that approach.
A calcium score of zero does not mean a person is permanently “immune” from heart disease, nor does it mean cholesterol should simply be ignored. However, in many individuals without detectable plaque, the absence of coronary calcium may suggest substantially lower short-term cardiovascular risk despite elevated cholesterol levels.(12)
In these situations, many experts now recommend individualized decision-making, aggressive lifestyle optimization, metabolic evaluation, and repeat follow-up imaging over time rather than reflexively treating cholesterol numbers alone as though they already represent established disease.
Importantly, advanced imaging is now identifying many individuals with elevated cholesterol who nevertheless show no evidence of detectable atherosclerosis. In some of these patients, the absence of coronary plaque may help avoid unnecessary statin therapy while allowing a more personalized, precision-based prevention strategy focused on metabolic health, inflammation, lifestyle improvement, and long-term monitoring.
This represents a major philosophical shift in cardiovascular prevention. Instead of automatically treating cholesterol as though it were the disease itself, physicians are increasingly using advanced imaging to first determine whether actual heart disease is present before deciding how aggressively a cholesterol-related risk factor should be treated.
Cholesterol may suggest risk. But imaging identifies disease. Modern prevention is increasingly shifting toward treating actual disease while still carefully monitoring future risk.
Treating the “Fire,” Not Just the “Sparks”
One of the easiest ways to understand modern heart disease is through the idea of “the fire and the sparks.”
Cholesterol may act like sparks entering the artery wall, but the underlying inflammatory and metabolic environment may be the fire allowing damage to continue.
If the artery remains inflamed because of insulin resistance, poor sleep, chronic stress, smoking, obesity, poor nutrition, lack of exercise, or metabolic dysfunction, then lowering cholesterol alone may not completely address the problem.
This is why many doctors now believe prevention must go beyond cholesterol reduction alone.
Importantly, even after LDL cholesterol improves, many patients continue to carry what doctors call “residual risk.” This may include residual inflammatory risk, residual thrombotic risk, residual triglyceride risk, residual lipoprotein(a) risk, residual metabolic risk, residual diabetes risk, and ongoing plaque-biologic risk despite improved cholesterol numbers.(5–15)
In other words, LDL cholesterol represents only one piece of a much larger cardiovascular puzzle.
The ultimate goal is not simply LDL reduction. The goal is cardiovascular risk reduction as a whole.
A healthier metabolic and inflammatory environment may help create healthier arteries, more stable plaque, and better long-term cardiovascular outcomes.
Lifestyle Still Matters Tremendously
Despite advances in medications and imaging, lifestyle remains one of the most powerful tools in cardiovascular prevention.
Nutrition, movement, sleep, stress reduction, weight management, smoking cessation, and metabolic health all strongly influence inflammation and vascular biology.
Regular physical activity improves insulin sensitivity, blood pressure, endothelial function, mitochondrial health, and inflammatory balance.(10,11)
Sleep is also critically important. Poor sleep has been linked to obesity, diabetes, inflammation, high blood pressure, abnormal stress hormones, and increased cardiovascular risk.
Chronic stress may continuously stimulate inflammatory and hormonal pathways that affect both metabolism and the arteries.
Importantly, insulin resistance itself does not simply appear “out of nowhere.” In many people, it gradually develops through the combined effects of chronic stress, inflammation, poor nutrition, excess processed foods, obesity, physical inactivity, poor sleep, hormonal imbalance, chronic illness, emotional stress, and even demanding work environments. Increased rates of metabolic dysfunction and cardiovascular disease have been observed in chronically high-stress professions such as first responders, police officers, emergency personnel, healthcare workers, and high-pressure financial occupations.
In many respects, lifestyle directly shapes the body’s metabolic terrain.
Even nutrition affects much more than cholesterol alone. Processed foods, excess sugars, unhealthy metabolic signaling, obesity, chronic stress, and sedentary behavior may all contribute to inflammatory activation and vascular injury over time.
Genetics may influence a person’s predisposition toward insulin resistance and cardiovascular disease, but lifestyle and environment strongly influence how those genetic tendencies are ultimately expressed. This interaction between genetics and environment, often referred to as epigenetics, helps explain why sleep, stress, exercise, nutrition, behavior, and overall lifestyle can profoundly affect long-term health outcomes.
This is why many experts now focus on improving the body’s overall biologic environment rather than concentrating only on one laboratory number.Top of Form
Bottom of Form
Functional and Preventive Medicine Perspectives
Functional and preventive medicine attempt to look upstream at the factors contributing to disease long before major cardiovascular events occur.
This includes evaluating nutrition, insulin resistance, metabolic health, inflammation, stress physiology, sleep quality, exercise habits, body composition, gut health, hormonal balance, micronutrient status, environmental exposures, recovery, and other biologic contributors that may influence chronic disease over time.
The purpose is not to replace traditional cardiology, but rather to complement it by helping patients better understand the underlying biologic terrain affecting their health.
In many cases, combining modern medical imaging and evidence-based treatment with proactive lifestyle and metabolic intervention may provide a more complete prevention strategy.
Importantly, metabolic functional medicine is not simply about “taking supplements.” At its core, it is a science-based attempt to better understand how the human body is designed to function, what drives health, what disrupts biologic balance, and why chronic disease develops over time.
This approach focuses on understanding upstream biologic pathways involving metabolism, inflammation, hormones, mitochondrial function, stress physiology, nutrition, sleep, exercise, detoxification systems, gut health, immune signaling, recovery, and cellular energy production. In many respects, it attempts to understand not only disease itself, but also the biology of wellness and resilience.
Because if we do not understand what healthy function looks like, it becomes much harder to fully understand what disease actually represents.
In this way, metabolic functional medicine views the body as an interconnected system rather than isolated organs functioning independently. The same biologic networks influencing energy, sleep, mood, metabolism, inflammation, hormones, and recovery also influence cardiovascular disease and long-term health outcomes.
This includes studying genetic predispositions, metabolic pathways, detoxification pathways, hormonal balance, circadian rhythms, mitochondrial function, fuel utilization, micronutrient status, inflammatory signaling, stress responses, and the gut microbiome in an effort to better understand how the body functions under both healthy and diseased conditions.
In many respects, practitioners of metabolic functional medicine act both as detectives and architects: detectives seeking to understand why disease developed in the first place, and architects working to help build a healthier biologic environment that may optimize wellness, resilience, recovery, and long-term function.
A useful analogy is maintaining a high-performance engine. Waiting until the engine completely breaks down before paying attention to maintenance is very different from proactively optimizing fuel quality, oil, cooling systems, performance, and long-term function over time. Similarly, proactive metabolic and preventive medicine attempts to identify dysfunction earlier, improve biologic efficiency, and optimize the body’s internal environment long before major disease events occur.
Increasingly, many physicians and scientists now recognize that understanding wellness biology may be just as important as understanding disease biology itself.
The Future of Heart Disease Prevention
The future of cardiovascular prevention will likely involve both modern medical treatment and a deeper understanding of the biologic forces driving disease.
Cholesterol still matters.
But heart disease is increasingly being recognized as much more than cholesterol alone.
Inflammation matters.
Metabolic health matters.
Insulin resistance matters.
Sleep matters.
Stress matters.
Lifestyle matters.
Plaque biology matters.
Most importantly, early prevention matters.
Heart disease often develops silently for years before symptoms appear. For many people, the first warning sign may unfortunately be a heart attack, a stent, bypass surgery, stroke, heart failure, or sudden loss of a loved one. By the time symptoms finally appear, the disease process has often already been developing quietly beneath the surface for decades.
The earlier people understand what is happening inside their arteries and inside their metabolism, the greater the opportunity to change the future before major damage occurs.
Cholesterol may suggest risk.
Imaging can identify disease.
Metabolic testing may help explain why the artery became unhealthy in the first place.
The goal is not simply lowering one laboratory number. The goal is reducing overall cardiovascular risk, improving long-term health, and helping people live longer, healthier, and more resilient lives.
A New Era of Prevention: Treating Disease, Biology, and Risk, Not Just Numbers
Heart disease rarely happens suddenly. In most people, it develops quietly over many years before symptoms ever appear.
Do not wait for a heart attack, stent, bypass surgery, stroke, heart failure, or diabetes diagnosis before taking your health seriously.
Modern cardiovascular prevention is evolving. We are no longer simply treating laboratory numbers as though the numbers themselves are the disease. Increasingly, medicine is recognizing that cholesterol is part of heart disease, but cholesterol itself is not the disease.
Atherosclerosis is the disease. Coronary artery disease is the disease. Plaque inside the artery wall is the disease… not cholesterol itself, and not even LDL alone.
Cholesterol is one important risk factor within a much larger biologic process involving inflammation, insulin resistance, metabolic dysfunction, oxidative stress, endothelial injury, thrombosis, lifestyle, genetics, and plaque biology.
The real goal is understanding what is happening inside the artery wall and inside the body long before major events occur.
That means understanding inflammation, insulin resistance, metabolic health, plaque biology, stress, sleep, nutrition, exercise, body composition, blood pressure, smoking, hormonal balance, and the overall biologic environment influencing vascular health over time.
Cholesterol may suggest risk.
Imaging can identify disease.
Metabolic testing may help explain why the disease developed in the first place.
This represents a major shift in medicine. Instead of simply reacting after disease becomes severe, modern prevention increasingly focuses on identifying disease earlier, understanding the upstream biologic drivers contributing to vascular injury, and reducing overall cardiovascular risk before catastrophic events occur.
At CardioCore Metabolic Wellness Center, the focus is on helping patients better understand the connection between heart disease, metabolism, inflammation, lifestyle, and overall biologic health through a more comprehensive and personalized approach to prevention and wellness.
The goal is not simply lowering LDL cholesterol.
The goal is reducing cardiovascular risk, improving metabolic health, optimizing biologic function, and helping people live longer, healthier, stronger, and more resilient lives.
About the Author
Dr. John Sciales is a cardiometabolic specialist whose work focuses on Functional Medicine, systems biology, patient education, and health coaching within an integrated cardiometabolic framework. Although he no longer practices traditional clinical medicine, his work centers on empowering both patients and physicians through a deeper understanding of cardiometabolic disease and its underlying biologic drivers.
Dr. Sciales emphasizes that meaningful improvement in chronic disease requires both accurate downstream evaluation according to established medical standards and targeted upstream intervention directed toward the biologic mechanisms contributing to disease development and progression. He helps patients understand whether disease has been properly identified, whether it is being managed according to current medical guidelines, and how underlying contributors involving nutrition, metabolism, targeted supplementation, stress physiology, sleep quality, mitochondrial health, inflammation, and the gut microbiome may be addressed in a structured and individualized manner.
Central to his philosophy is the recognition that upstream drivers of disease cannot be effectively addressed without accurate downstream assessment. Accordingly, he coaches patients to engage more effectively with their physicians, enabling more informed, collaborative discussions and improved alignment of care. His unique perspective arises from integrating conventional medical understanding of disease identification, imaging, risk stratification, and evidence-based standards of care with a broader Functional Medicine approach focused on the inflammatory-metabolic terrain underlying chronic disease progression.
Dr. Sciales actively supports communication with his clients’ physicians and welcomes interdisciplinary collaboration when appropriate to enhance the quality, continuity, and precision of care. All communications with clients and, when appropriate, their physicians are grounded in and supported by relevant medical literature, helping ensure that recommendations remain aligned with current evidence and standards of care.
His overarching goal is to help individuals with chronic cardiometabolic dysfunction move beyond reactive disease management toward optimized metabolic health, biologic resilience, and long-term wellness through an integrated, systems-based approach to cardiometabolic medicine.
CLICK HERE TO BOOK A DISCOVERY CALL
CLICK HERE TO JOIN OUR PRIVATE CardioCore COMMUNITY
CLICK HERE TO SPEAK TO OUR VIRTUAL ASSISTANT
References
Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from randomized trials. Lancet. 2015;385:1397–1405.
American College of Cardiology/American Heart Association Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2014;129:S1–S45.
Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713–1722.
Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387–2397.
Ridker PM, Everett BM, Thuren T, et al. Anti-inflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377:1119–1131.
Tardif JC, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381:2497–2505.
Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in patients with chronic coronary disease. N Engl J Med. 2020;383:1838–1847.
Libby P. Inflammation in atherosclerosis. Nature. 2002;420:868–874.
Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364:226–235.
Reaven GM. Banting Lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37:1595–1607.
Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome. Circulation. 2009;120:1640–1645.
Hecht HS, Blaha MJ, Kazerooni EA, et al. CAC scoring: clinical indications and interpretation. JACC Cardiovasc Imaging. 2017;10:923–937.
Ridker PM, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195–2207.
Bhatt DL, Steg PG, Miller M, et al. Cardiovascular risk reduction with icosapent ethyl. N Engl J Med. 2019;380:11–22.
Budoff MJ, Bhatt DL, Kinninger A, et al. Effect of icosapent ethyl on progression of coronary atherosclerosis in patients with elevated triglycerides on statin therapy: EVAPORATE trial. Eur Heart J. 2020;41:3925–3932.
DeFronzo RA. Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis. Diabetologia. 2010;53:1270–1287.
Nissen SE, Nicholls SJ, Sipahi I, et al. Effect of intensive statin therapy on progression of coronary atherosclerosis. JAMA. 2006;295:1556–1565.
