Why Cholesterol and Blockages Don’t Tell the Whole Story What Really Causes Heart Attacks?
Beyond Blockages: What Really Causes Heart Attacks
Why “The Lumen Is Not the Disease”
Dr. John Sciales
Director: CardioCore Metabolic Wellness Center
The Number That Scares Everyone
It often begins with a number.
A patient sits in a doctor’s office and hears something like, “You have a 70% blockage.” Sometimes it is even higher, 80% or 90%. The reaction is immediate. Fear sets in. The assumption feels obvious: the larger the blockage, the closer you must be to a heart attack.¹
Or maybe you are told, “It’s not too bad. You don’t need a stent. It’s less than 50% blockage.” That may sound reassuring. But does that really mean everything is fine?
For decades, heart disease has been explained in this simple way. Arteries are like pipes. Over time, they slowly fill with buildup. The more clogged they become, the more dangerous the situation.
And there is some truth to this. When a blockage becomes severe, usually above 70%, it can reduce blood flow. This can lead to chest pain, especially during activity. In those situations, placing a stent can help improve blood flow and relieve symptoms.²
But there is an important part of the story that most people are never told.
The size of the blockage is only part of the picture.
What may matter even more is what is happening beneath the surface of the plaque itself. Is the plaque stable and quiet, or inflamed and unstable? Some plaques may appear smaller on the inside of the artery but are actually more dangerous because they are biologically active and more likely to rupture.³⁻⁵
That hidden biology is often far more important than the percentage of blockage alone.
The Truth That Changes Everything
Here is what surprises many people.
Most heart attacks do not come from severe blockages.³⁻⁶
Many heart attacks occur in arteries that were only 30% to 50% blocked before the event. That means the blockage that looks the most dangerous on a test is often not the one that causes the heart attack.³⁻⁶
Why?
Because heart attacks are usually caused by the sudden rupture of an unstable plaque hidden within the artery wall. When that plaque ruptures, the body reacts as if there has been an injury. A blood clot quickly forms over the rupture and can suddenly block blood flow, causing a heart attack.⁴⁻⁷
So the real danger is not always the biggest blockage.
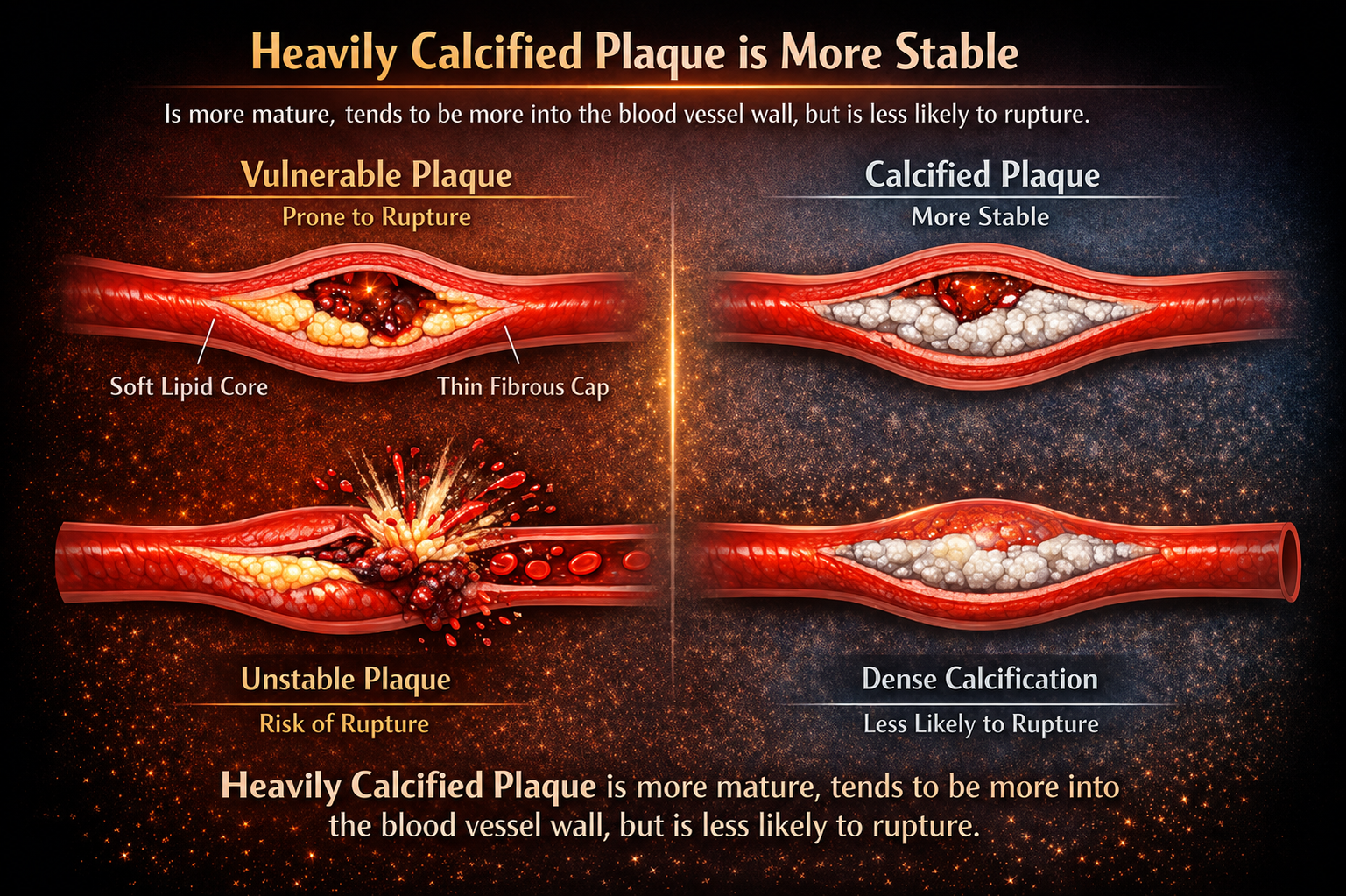
Older plaques have often had more time to heal, harden, and calcify. These plaques are usually more stable and less likely to rupture. Younger, softer plaques are often more inflamed and biologically active. They are more unstable and more likely to suddenly rupture.⁴⁻⁸
That does not mean calcified plaque is “good.” It still means heart disease is present. But softer, inflamed plaque may actually be more dangerous than a larger, heavily calcified plaque.⁴⁻⁸
This is why plaque biology matters so much.
The question is not only:
“How big is the blockage?”
The more important question is:
“What type of plaque is it, and how likely is it to rupture?”⁴⁻⁹
Heart disease is not just a plumbing problem.
It is a biologic process happening within the artery wall.³⁻¹⁰
Why Opening Arteries Doesn’t Always Prevent Heart Attacks
However, in 2007, a major study called the COURAGE Trial helped answer this question.¹¹
Researchers studied patients with stable symptomatic heart disease. One group received stents along with medication, while the other group received medication alone without stenting or revascularization.¹¹
The results surprised many doctors.
Although stents improved symptoms like chest pain, called angina, they did not significantly reduce heart attacks or death compared to medication alone.¹¹
This became a major turning point in how we understood heart disease.
Improving symptoms matters. Helping someone walk farther, exercise more comfortably, or live with less chest pain can greatly improve quality of life. But the ultimate goal of treatment is not simply symptom relief. The true goal is to prevent heart attacks, preserve heart muscle, and reduce death.
At first, this seemed confusing.
Large blockages clearly reduce blood flow. During exercise or physical stress, they may cause chest pain or angina. Opening those blockages with a stent can improve circulation and help patients feel better. So why were these severe blockages not always the main cause of heart attacks?
The answer began to change the entire way we viewed heart disease.
Many large plaques are older plaques. Over time, they often become more calcified, more stable, and less likely to suddenly rupture. In contrast, smaller plaques may not significantly block blood flow, yet they are often softer, more inflamed, and biologically unstable.³⁻⁸
And unstable plaque is dangerous.
When one of these plaques suddenly ruptures, the body reacts as if there has been an injury. A clot rapidly forms over the rupture site, sometimes blocking blood flow within minutes and causing a heart attack without warning.⁴⁻⁷
Because the blockage occurs so suddenly, the body has little time to adapt. Blood flow is abruptly cut off, often leading to more severe damage to the heart muscle and, in many cases, higher death rates.
By comparison, when an artery slowly narrows over many years, the body may gradually develop tiny natural bypass vessels called collateral circulation. These vessels can sometimes help preserve blood flow around the blockage.¹²
And this led to another surprising realization.
In many cases, the more severe and slowly developing blockages may actually cause less severe heart attacks because the body has had time to partially compensate. These events are often smaller and are commonly called NSTEMIs, or non-ST elevation heart attacks.
In contrast, milder but unstable plaques may suddenly rupture and completely block an artery within minutes, causing far more catastrophic injury to the heart muscle. These are often the large, sudden heart attacks known as STEMIs, or ST-elevation myocardial infarctions.⁴⁻⁷
This was another important clue.
Heart attacks are not determined only by how narrow an artery becomes.
They are driven by the biology and behavior of the plaque hidden within the artery wall.³⁻¹⁰
The Disease You Cannot See
Most people think of heart disease as a plumbing problem. A pipe slowly fills with debris until it eventually becomes blocked.
But the human body is far more intelligent than that.
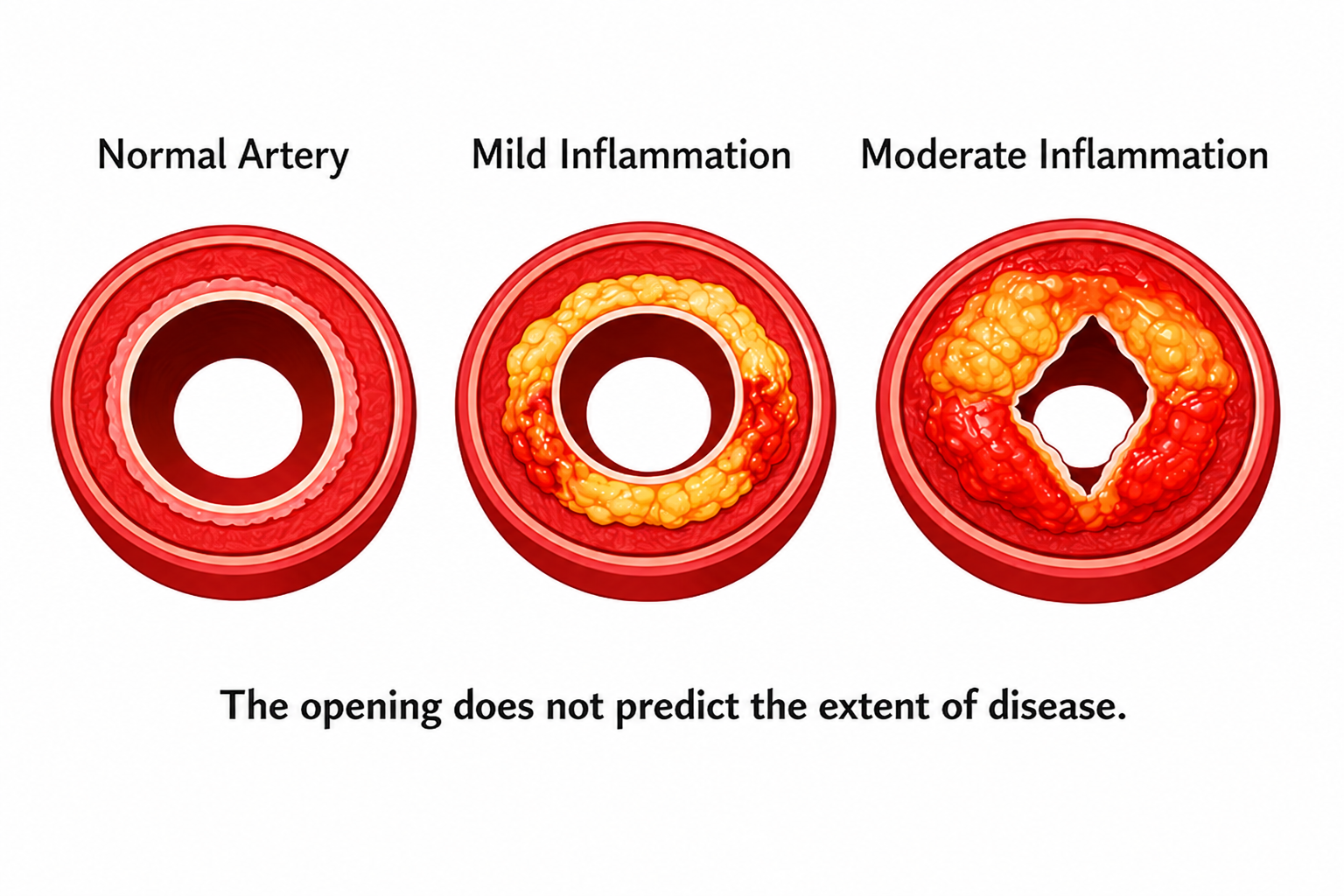
In the early stages of heart disease, plaque does not simply grow inward and clog the artery. Instead, the artery often expands outward to make room for the plaque while keeping blood flow relatively normal.¹³⁻¹⁵
This is one of the reasons heart disease can remain silent for so many years.
From the inside, the opening of the artery, called the lumen, may still look relatively normal. Blood continues to flow. Everything appears fine. In fact, the opening of the lumen is what doctors are measuring when you are told that a blockage is 30%, 50%, or even 90%. It is not measuring the total amount of plaque hidden within the artery wall.¹³⁻¹⁵
But beneath the surface, the disease may already be growing like a smoldering volcano hidden within the artery wall.
Imagine your kitchen drain. Normally, you would expect debris to slowly build up and narrow the opening. But now imagine the pipe quietly stretching outward as the buildup grows. From the inside, the opening still appears normal. Water continues to flow. Everything seems fine.
Yet underneath the surface, the problem is becoming larger and more dangerous.
This is exactly what happens inside many arteries.
Long before a major blockage appears, plaque may already be silently building within the artery wall while the vessel expands outward to compensate. A person may feel perfectly healthy, have no symptoms, and even have normal testing, while heart disease continues progressing quietly beneath the surface.¹³⁻¹⁵
The Glagov Effect: How the Body Hides Disease
This process is called the Glagov effect.¹³
It describes how arteries expand outward during the early stages of plaque buildup in an attempt to preserve blood flow. In many ways, the body is trying to protect you and compensate for the growing disease.
As plaque slowly builds within the artery wall, the vessel stretches outward so the inner opening, the lumen, can remain relatively unchanged. This means a person may already have a significant amount of plaque hidden within the artery wall without any major visible blockage.¹³⁻¹⁵
Heart disease may already be present even when the artery still appears “normal” from the inside.
Only later, when the artery can no longer expand outward, does the plaque begin pushing inward into the lumen. That is when the blockage finally becomes visible on testing.
By the time someone is told they have a 70% blockage, the disease has often been silently developing for many years, and sometimes even decades.
This is why focusing only on blockage can be misleading.
The disease begins long before we can clearly see it.
Understanding Plaque: What’s Really Inside the Artery
To understand heart disease, we must first understand plaque.
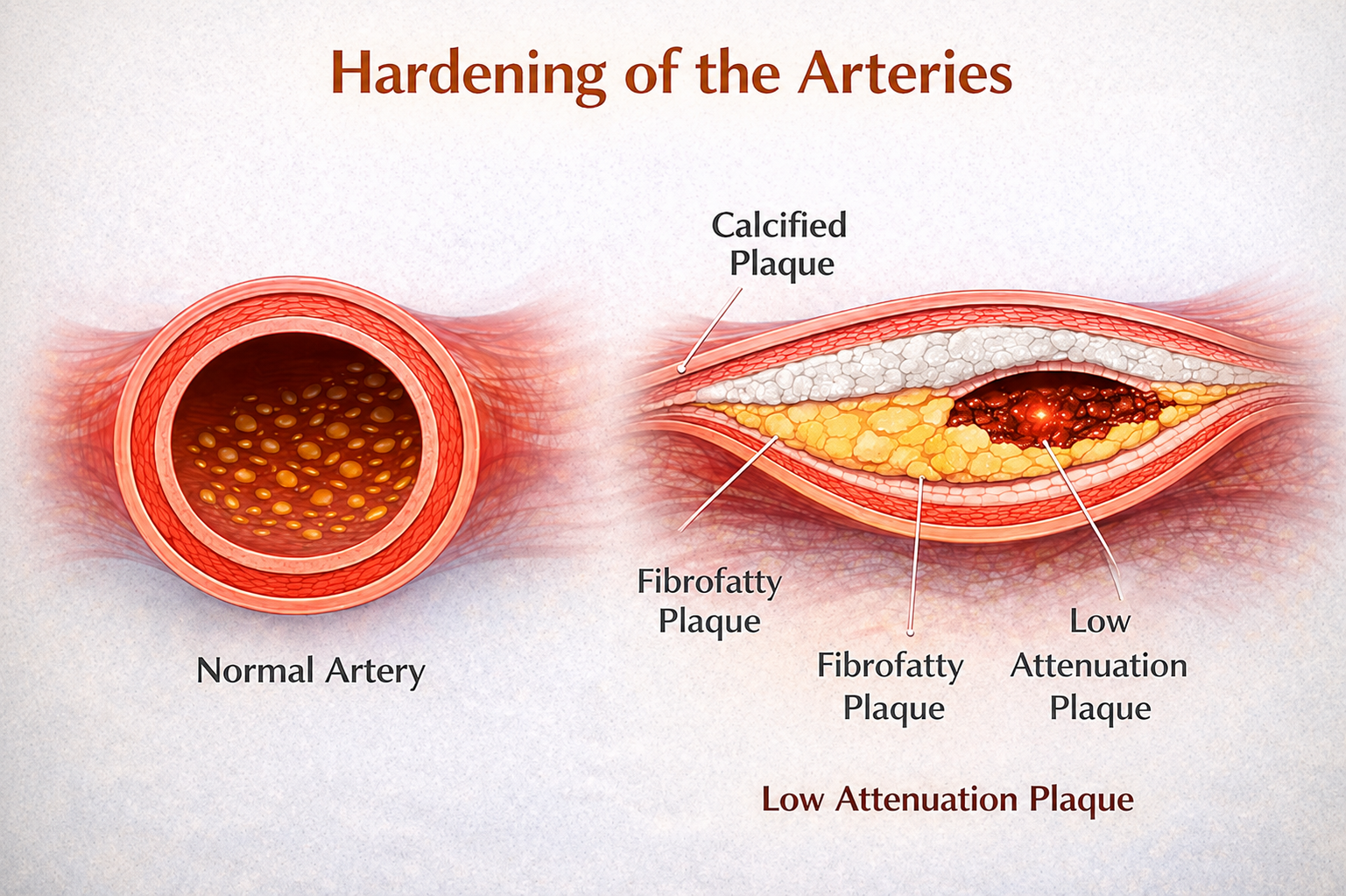
Plaque is not just a single substance. It has different layers, different compositions, and different behaviors.
There is the total amount of plaque hidden within the artery wall. Within that are areas of fibrofatty plaque, which make up much of the bulk of the buildup. And within those areas may be low attenuation plaque, the most dangerous type of plaque.
Low attenuation plaque is softer, more inflamed, and biologically unstable. It is the type most likely to suddenly rupture and trigger a heart attack.³⁻⁹
In many ways, plaque behaves less like simple “clogging” and more like a living biologic process occurring inside the artery wall.
The Chernobyl Analogy: Looking Beneath the Surface
To better understand this, imagine the Chernobyl disaster.
After the reactor accident, the damaged nuclear core was buried beneath massive layers of concrete. Think of the calcium covering plaque in a similar way. The calcified outer layer is like the concrete cap that can be seen on imaging studies projecting into the lumen.
Beneath that lies the fibrofatty plaque, similar to the buried nuclear waste itself.
But the most important question is not simply how much “waste” is there.
The real question is:
“What is the biologic activity beneath the surface?”
That is what low attenuation plaque represents.⁴⁻⁹
It reflects how “hot,” inflamed, biologically active, and unstable the plaque is beneath the surface. Two people may have similar amounts of plaque, yet one person’s plaque may be far more dangerous because it is more inflamed and more likely to rupture.⁴⁻⁹
Just as buried nuclear material can remain dangerous beneath a concrete shell, plaque may appear stable on the surface while dangerous inflammation continues underneath.
Why Plaque Biology Matters More Than Blockage
This is why measuring the amount of lumen blockage, also called “percentage stenosis,” is only part of the story. Although it remains important for estimating risk and determining whether blood flow may be limited, it does not fully define how dangerous plaque may be.¹⁻³
Two people may have similar degrees of blockage, yet one may have relatively stable plaque while the other has highly inflamed, unstable plaque that is far more likely to rupture.⁴⁻⁹
And that rupture is what often causes the heart attack.
When unstable plaque suddenly tears open, the body reacts as if there has been an injury. A blood clot rapidly forms over the rupture site, and within minutes that clot can suddenly block the artery completely.⁴⁻⁷
This is why a smaller blockage can sometimes be far more dangerous than a larger one.
The real issue is not simply how narrow the artery appears.
The real question is:
👉 “What type of plaque is present, and how unstable is it?”
The future of heart disease is not simply measuring how narrow the artery becomes.
It is understanding the biology hidden beneath the surface.
What We Learned from the EVAPORATE Trial
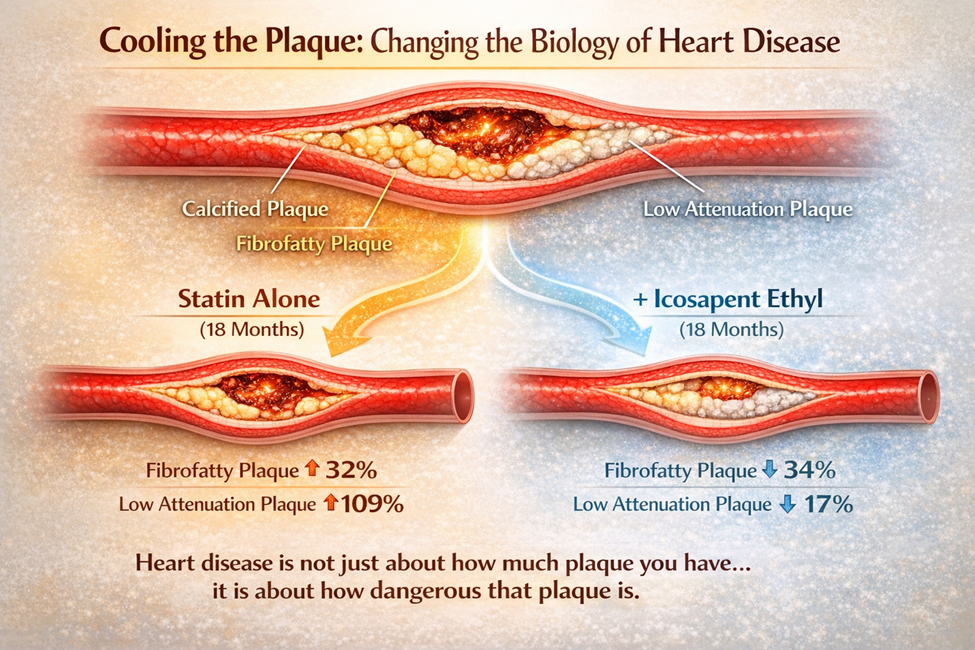
A study called the EVAPORATE Trial provided important insight into plaque behavior.¹⁶⁻¹⁷
Patients in this study were already taking high-intensity statins, which are medications known to lower cholesterol and reduce cardiovascular risk. In fact, since 2013, treatment guidelines for significant plaque have emphasized high-intensity statin therapy rather than simply using lower doses because “the cholesterol number looks good.”¹⁸
But when researchers closely examined plaque over 18 months, they found something unexpected.
Even while taking high-intensity statins, fibrofatty plaque still grew, increasing by about 32%. More concerning, low attenuation plaque, the most dangerous and unstable type of plaque, increased by about 109%.¹⁶⁻¹⁷
This was an important realization.
Even with good cholesterol control, dangerous plaque biology could still continue to progress.
Then a second treatment was added: icosapent ethyl, a highly purified omega-3 derived from fish oil. This is not the same as over-the-counter fish oil. It is a refined, medical-grade therapy, similar to how crude oil is refined into jet fuel.
With this addition, the results were very different.
Over the same 18 months, fibrofatty plaque decreased and shrank by about 34%, while low attenuation plaque decreased by about 17%.¹⁶⁻¹⁷
In other words, the dangerous plaque became less biologically active and less unstable.
And perhaps most importantly, this occurred without any additional lowering of LDL cholesterol levels.¹⁶⁻¹⁷
This suggested something profound:
Heart disease is not driven by cholesterol alone.
Plaque biology, inflammation, and plaque behavior matter too.
And this raises an important question for many people:
If my cholesterol looks “good,” and I am taking a statin, what is actually happening to my plaque?
Is it growing or shrinking?
Is it becoming more stable and less dangerous?
Or is dangerous plaque biology still progressing quietly beneath the surface?
In other words, which group are you in?
Without looking directly at the arteries and understanding plaque behavior, we may not fully know the answer.
Cholesterol: Essential but Incomplete
For many years, cholesterol has been portrayed as the main cause of heart disease. But the reality is far more complex.
Cholesterol is not simply a “bad” substance. It is essential for life. The body uses cholesterol to build cell membranes, produce hormones, support brain function, and help generate energy within cells. In certain situations, cholesterol may even play protective and anti-inflammatory roles.
So cholesterol itself is not the enemy.
The real problem begins when cholesterol exists within an inflamed and unhealthy biologic environment. In that setting, cholesterol can become oxidized, penetrate the artery wall, and contribute to plaque formation and instability.¹⁹⁻²²
This helps explain something that has confused both patients and doctors for years.
Some people live long, healthy lives despite elevated cholesterol levels, while others develop significant heart disease even when their cholesterol appears “normal” or only mildly elevated.
There are certainly forms of heart disease that are strongly driven by cholesterol, especially conditions like familial hyperlipidemia, where LDL cholesterol levels are extremely elevated from an early age and clearly contribute to accelerated plaque formation.²³
But that is not the whole story.
Many people develop significant heart disease despite having normal or only mildly elevated cholesterol levels. In these individuals, the disease may be driven more by chronic inflammation, insulin resistance, metabolic dysfunction, thrombosis, elevated lipoprotein(a), triglyceride-rich particles, or other biologic processes occurring within the artery wall.²⁰⁻²⁶
The Modern Cardiometabolic Environment
Over the last several decades, smoking rates have declined significantly across much of the developed world. Yet during that same period, rates of obesity, insulin resistance, metabolic syndrome, visceral adiposity, fatty liver disease, sedentary behavior, sleep dysfunction, ultra-processed food consumption, chronic stress, and type 2 diabetes have risen dramatically.²⁴⁻²⁹
The modern cardiovascular environment has changed.
Atherosclerosis increasingly appears to represent far more than a simple cholesterol-storage disorder. Instead, growing evidence suggests it reflects the structural expression of chronic endothelial injury occurring within a complex inflammatory and cardiometabolic environment.²⁰⁻²⁶
Inflammation, insulin resistance, oxidative stress, endothelial dysfunction, mitochondrial dysfunction, thrombogenicity, autonomic imbalance, and altered plaque biology now appear to play major roles in plaque progression and plaque instability, often independent of LDL cholesterol levels alone.²⁰⁻²⁶
This may help explain one of the central paradoxes of modern cardiology:
Despite aggressive LDL lowering, substantial cardiovascular risk still remains.²⁷⁻³⁰
Why “Normal Cholesterol” Can Be Misleading
Many people assume that a normal cholesterol level means they are safe from heart disease.
But that is not always true.
A large percentage of individuals who experience heart attacks have cholesterol levels that fall within the “normal” range.³¹
So when someone is told, “Your cholesterol is fine,” it may sound reassuring, but it does not necessarily mean their arteries are healthy.
Cholesterol is a surrogate marker. It provides indirect information about risk, but it does not directly show us the artery wall itself. It does not tell us how inflamed the body is, how unstable plaque may be, or what is actually happening beneath the surface.
A cholesterol number may estimate risk.
But it does not define disease.
Why Plaque Biology Matters
This is why plaque biology has become so important.
If someone develops significant atherosclerosis despite relatively normal cholesterol levels, is the disease truly being driven primarily by LDL cholesterol alone?
Or is inflammation playing a much larger role than we once realized?
And this forces us to ask an even bigger question:
Are we truly treating cardiovascular risk reduction?
Or are we mainly treating cholesterol reduction?
Because real cardiovascular prevention should not simply focus on lowering a laboratory number. It should focus on reducing the actual biology that drives plaque progression, plaque instability, heart attacks, disability, and death.²⁰⁻²⁶
Plaque biology allows us to look beyond cholesterol numbers alone and better understand the inflammatory activity occurring within the artery wall itself. Two people may have similar cholesterol levels, yet one may have relatively stable plaque while the other has highly inflamed, biologically active plaque that is far more dangerous.⁴⁻⁹
This is why having a “good cholesterol number” is not always reassuring.
The arteries may still be silently exposed to inflammation and metabolic dysfunction long before a heart attack ever occurs.
The future of heart disease is not simply understanding cholesterol.
It is understanding the biology hidden beneath the surface.
Changing Biology to Change Outcomes
When we better understand the biology of heart disease, we gain the ability to influence it.
We can reduce inflammation, improve metabolic health, stabilize plaque, and decrease the likelihood of plaque rupture.²⁰⁻²⁶
And when we change these underlying biologic processes, we change outcomes.
That is the true goal of prevention.
Waiting for disease to progress to the point where we must mechanically open an artery with a stent or bypass surgery is not true prevention. That is reacting to advanced disease after years of silent progression.
The Reality of Recurrence
Even after procedures like stents or bypass surgery, the risk does not disappear.³²⁻³⁴
Within five years, a significant percentage of patients will experience another major cardiac event. And very often, that event does not come from the original blockage that was treated.³²⁻³⁴
Instead, it frequently comes from a different plaque in another part of the artery system, one that may not have appeared severe enough to treat at the time.³⁻⁶
This reveals an important truth.
Heart disease is not simply a problem of one blockage.
It is a disease of the entire arterial system and the biologic environment affecting those arteries.
The Hidden Warning Signs of Cardiometabolic Disease Hiding in Plain Sight
One of the biggest problems in modern medicine is that disease may be developing long before traditional testing becomes obviously abnormal.
A person may be told their cholesterol is “acceptable,” their blood sugar is “normal,” and their stress test is “fine,” yet dangerous plaque may still be silently developing within the artery wall.
Which raises an important question:
Are “normal” labs always truly normal?
This is because cardiometabolic disease often begins years, and sometimes decades, before symptoms appear. The warning signs are often hiding in plain sight.
But if we do not look for them, do not understand them, or choose to ignore them, we may never see the disease developing beneath the surface until catastrophe occurs.
These are some of the most common warning signs hiding in plain sight:
Borderline blood sugar. “Prediabetes.” Or established diabetes mellitus.²⁴⁻²⁹
Elevated triglycerides, especially above 100. Low HDL cholesterol or an elevated triglyceride-to-HDL ratio (>2.5), often suggesting underlying insulin resistance long before diabetes is diagnosed.²⁴⁻²⁹
The slowly expanding waistline and visceral fat accumulating deep within the abdomen.²⁴⁻²⁹
Fatty liver disease. High blood pressure.²⁴⁻²⁹
And often overlooked “non-disease” contributors that still strongly influence disease biology: poor sleep, chronic stress, exhaustion, sedentary living, and loss of physical conditioning.²⁵⁻²⁹
And frequently, a powerful family history of early heart disease, stroke, or diabetes.
Certain ethnic groups may face even greater vulnerability. Many South Asian, Hispanic, Middle Eastern, and other populations often develop insulin resistance, metabolic syndrome, fatty liver disease, and premature cardiovascular disease at much lower body weights than traditionally expected.²⁸⁻³⁰
These are not isolated findings.
They are clues that the metabolic and inflammatory terrain of the body may already be shifting toward endothelial dysfunction, plaque instability, and accelerated vascular disease long before a heart attack occurs.²⁰⁻²⁶
This is why plaque biology matters so much.
Plaque helps reveal what kind of biologic environment is developing within the artery wall itself. But to truly understand cardiovascular risk, we must also look beyond the artery and understand the person carrying the disease, including their metabolic health, inflammation, body composition, lifestyle, stress, sleep, genetics, ethnicity, and overall cardiometabolic environment.
Heart disease is not simply a blockage problem.
It is often the structural expression of a much deeper biologic process occurring throughout the entire body.
Why Stress Testing Has a Limited Role in Detecting Heart Disease
The Limitations of Stress Testing
For many years, stress testing has been one of the most commonly used tools in cardiology. It is widely available, performed in the office, and can help determine whether a patient has a major blockage that significantly limits blood flow.
But it is important to understand what a stress test actually measures, and more importantly, what it does not.
A stress test primarily evaluates the lumen, the inside opening of the artery. It is designed to detect large, flow-limiting blockages, typically those narrowing an artery by 70% or more. These are the types of blockages that may reduce blood flow enough to cause chest pain or shortness of breath during exercise.² ¹¹
In that situation, stress testing can be very useful.
But as we have discussed throughout this article, most heart attacks do not come from these large, obvious blockages.³⁻⁶
They often arise from smaller plaques, sometimes only 30% to 50%, that are inflamed, unstable, and prone to rupture. These plaques may not significantly reduce blood flow and therefore may not appear abnormal on a stress test.³⁻⁹
This means a person can have a “normal” stress test and still have significant and potentially dangerous plaque developing silently within the artery wall.
And this is the major limitation of stress testing.
It tells us about the opening of the artery.
It tells us very little about the biology hidden within the artery wall itself.
In many ways, stress testing is looking at the wrong side of the concrete.
It evaluates whether the lumen has become severely narrowed, but it cannot see the dangerous plaque hidden beneath the surface, the inflammation, the fibrofatty plaque, or the low attenuation plaque that may be most likely to rupture.⁴⁻⁹
So stress testing answers a relatively narrow question:
“Is there a blockage severe enough to reduce blood flow right now?”
But it does not answer the deeper and often more important questions:
How much plaque is actually present?
What type of plaque is it?
Is the plaque stable or vulnerable?
What is this person’s future cardiovascular risk?
To answer those questions, we must move beyond simply looking for obstruction and begin directly imaging the arteries themselves.
Seeing the Entire Artery — And the Risk Beneath the Surface
Coronary CT angiography (CCTA), especially when combined with advanced plaque analysis, allows us to directly visualize the artery wall in far greater detail.³⁵⁻³⁸
Instead of simply asking whether blood flow is reduced, CCTA allows us to see the entire artery and better understand the risk hidden beneath the surface. It can identify total plaque burden, characterize fibrofatty and low attenuation plaque, and provide insight into plaque biology and future cardiovascular risk.³⁵⁻³⁸
This represents a major shift in cardiovascular medicine.
We are moving beyond simply looking at the lumen and asking whether an artery is obstructed.
We are beginning to understand the actual disease developing within the artery wall itself.
In the end, stress testing often tells us when we need to react.
But imaging the entire artery helps tell us how to prevent.
The Final Takeaway
A severe blockage may cause symptoms.
But a smaller, unstable plaque is often more likely to cause a heart attack.³⁻⁷
A normal cholesterol level may sound reassuring.
But it does not guarantee protection.³¹
The real issue is not simply what we see inside the opening of the artery.
The real danger may be the biologic activity developing silently within the artery wall itself.
The Truth That Changes Everything
Heart disease is not just about blockages or cholesterol.
It is about biology.
For decades, cardiology focused primarily on the opening of the artery, the lumen, measuring how narrow it became and reacting once blood flow was significantly reduced. But the lumen is not the disease. The disease lives within the artery wall itself, shaped by inflammation, metabolic dysfunction, endothelial injury, oxidative stress, plaque instability, thrombogenicity, and the overall biologic environment silently affecting the arteries years before symptoms ever appear.²⁰⁻²⁶
And when we begin to understand that, everything changes.
We stop simply reacting to advanced disease after catastrophe occurs and begin understanding how to truly prevent it in the first place.
To truly optimize cardiovascular risk reduction, rather than simply lowering cholesterol numbers, we must look much deeper. The goal is not merely to lower a laboratory value. The goal is to reduce the actual biologic processes driving plaque progression, plaque instability, heart attacks, heart failure, disability, and premature death.²⁰⁻²⁶
This is why residual risk matters so much.
Residual inflammatory risk.
Residual metabolic risk.
Residual thrombotic risk.
Residual triglyceride risk.
Residual lipoprotein(a) risk.
These hidden drivers may continue fueling disease even when cholesterol appears “controlled.”²⁰⁻³⁰
And this is why plaque biology tells us so much more of the story. It allows us to look beneath the surface and better understand the actual disease process occurring within the artery wall itself, helping us move beyond simply treating obstruction and toward understanding the terrain that creates disease in the first place.
The future of cardiovascular prevention is not simply about lowering cholesterol.
It is about understanding biology.
Now is the time to look deeper.
Now is the time to look beneath the surface.
Now is the time to act.
To learn more or schedule a complimentary discovery call with Dr. John and the CardioCore team, visit CardioCore Metabolic Wellness Center.
About the Author
Dr John Sciales is the founder of CardioCore Metabolic Wellness Center. His work focuses on helping people understand what is really driving heart disease, diabetes, weight gain, high blood pressure, fatigue, and other chronic health problems before serious events happen.
Dr. John believes that heart attacks, strokes, and chronic disease usually do not happen suddenly. They develop quietly over many years through problems like insulin resistance, inflammation, poor sleep, stress, unhealthy eating, lack of movement, hormone imbalance, and gut health problems.
His goal is to help people better understand their bodies, their risks, and the biology behind their health issues, not just treat numbers on a lab report. Using advanced heart imaging, metabolic testing, inflammation testing, and personalized lifestyle strategies, he helps patients look deeper at what may be happening beneath the surface.
Dr. John does not replace a patient’s doctor. Instead, he works alongside patients and their healthcare teams to provide education, guidance, and a more complete understanding of health and prevention. He strongly believes that combining modern medical evaluation with nutrition, lifestyle, metabolic health, and prevention offers a more proactive approach to long-term wellness.
Through CardioCore, his mission is simple: to help people identify problems earlier, better understand their health, and take control before disease becomes a crisis, through a more holistic, natural, and truly functional medicine approach.
References
Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316(22):1371–1375.
Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503–1516.
Little WC, Constantinescu M, Applegate RJ, et al. Can coronary angiography predict the site of a subsequent myocardial infarction in patients with mild-to-moderate coronary artery disease? Circulation. 1988;78(5 Pt 1):1157–1166.
Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47(8 Suppl):C13–C18.
Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circulation. 1995;92(3):657–671.
Ambrose JA, Tannenbaum MA, Alexopoulos D, et al. Angiographic progression of coronary artery disease and the development of myocardial infarction. J Am Coll Cardiol. 1988;12(1):56–62.
Libby P. Inflammation in atherosclerosis. Nature. 2002;420(6917):868–874.
Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies. Circulation. 2003;108(14):1664–1672.
Motoyama S, Kondo T, Sarai M, et al. Multislice computed tomographic characteristics of coronary lesions in acute coronary syndromes. J Am Coll Cardiol. 2007;50(4):319–326.
Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695.
Boden WE, O’Rourke RA, Teo KK, et al. COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503–1516.
Seiler C. The human coronary collateral circulation. Heart. 2003;89(11):1352–1357.
Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316(22):1371–1375.
Pasterkamp G, Schoneveld AH, van der Wal AC, Borst C. The relation of arterial geometry with luminal narrowing and histological markers for plaque vulnerability. Eur Heart J. 1998;19(12):1881–1887.
Schoenhagen P, Ziada KM, Vince DG, Nissen SE, Tuzcu EM. Arterial remodeling and coronary artery disease: the concept of “dilated” versus “obstructive” coronary atherosclerosis. J Am Coll Cardiol. 2001;38(2):297–306.
Budoff MJ, Bhatt DL, Kinninger A, et al. Effect of icosapent ethyl on progression of coronary atherosclerosis in patients with elevated triglycerides on statin therapy: EVAPORATE Trial. Eur Heart J. 2020;41(40):3925–3932.
Budoff MJ, Bhatt DL, Kinninger A, et al. Coronary plaque progression with icosapent ethyl versus placebo in statin-treated patients: EVAPORATE. Cardiovasc Res. 2020;116(13):e214–e216.
Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Circulation. 2014;129(25 Suppl 2):S1–S45.
Goldstein JL, Brown MS. A century of cholesterol and coronaries: from plaques to genes to statins. Cell. 2015;161(1):161–172.
Ridker PM. Inflammation, C-reactive protein, and cardiovascular disease: moving past the marker versus mediator debate. Circ Res. 2014;114(4):594–595.
Steinberg D. Low density lipoprotein oxidation and its pathobiological significance. J Biol Chem. 1997;272(34):20963–20966.
Libby P, Ridker PM, Hansson GK. Inflammation in atherosclerosis: from pathophysiology to practice. J Am Coll Cardiol. 2009;54(23):2129–2138.
Nordestgaard BG, Chapman MJ, Humphries SE, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated. Eur Heart J. 2013;34(45):3478–3490.
Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595–1607.
Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28(4):629–636.
Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860–867.
Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131.
Joshi P, Islam S, Pais P, et al. Risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA. 2007;297(3):286–294.
Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428.
Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (INTERHEART study). Lancet. 2004;364(9438):937–952.
Sachdeva A, Cannon CP, Deedwania PC, et al. Lipid levels in patients hospitalized with coronary artery disease. Am Heart J. 2009;157(1):111–117.e2.
Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials. Circulation. 2007;115(17):2344–2351.
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009
